SVT stands for Supraventricular Tachycardia. A Tachycardia means fast heartbeat. Supraventricular means it originates from somewhere above the ventricles i.e. in the atria or top chambers of the heart.
SVT usually refers to regular fast heart rhythms, as opposed to AF (which is technically still an SVT), which is irregular. This classification is useful, as SVTs are usually benign as opposed to heart rhythm disorders from the ventricles, which are not always.
There are three main types of SVT:
- Atrioventricular reentrant tachycardia (AVRT) – (also known as orthodromic reentrant tachycardia (ORT), or antidromic tachycardia depending on which direction it travels)
- Atrioventricular nodal reentrant tachycardia (AVNRT)
- Atrial tachycardia
SVTs are common in young people, particularly AVRT, which is most often seen in children and adolescents. AVNRT and atrial tachycardia are more often seen in middle-aged or elderly people. They are all due to a single abnormal electrical short circuit within the heart or from an abnormal focus of electricity.
More information:
AVRT – (or orthodromic reentry)
AVRT is an abnormal reentry circuit that occurs in people born with an extra or ’accessory’ pathway between the atria (A) and the ventricles (V). In most people there is only route from the atria to the ventricles, which is via the AV node, which lies in the middle of the heart. Accessory pathways are formed when the heart is growing as an embryo. The atria and ventricles usually separate during this process leaving the AV node as the only electrical connection between these chambers. However, in about 1 in every 700-1000 people, small strands of tissue are left between these chambers, and they can conduct electricity. As there are two routes between the atria and ventricles, electricity can conduct down one and back up the other, and so on, leading to a short circuit, or ‘reentry’ (see figure).
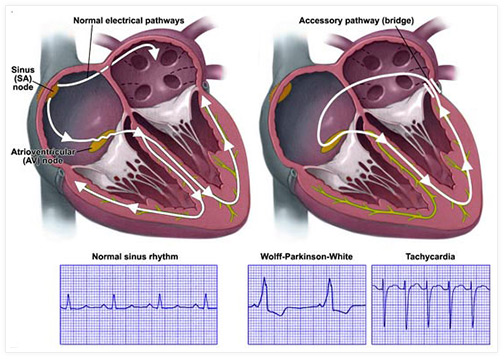
When electricity conducts down the AV node and back up the accessory pathway (as in the diagram above on the right), it is known as orthodromic reentrant tachycardia (ORT) and when it goes in the opposite direction it is called antidromic tachycardia. ORT is much more common than antidromic tachycardia. They have different ECG appearances but are otherwise treated in much the same way.
AVNRT
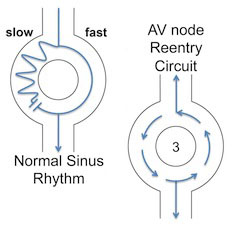
In 75% of the population, the AV node effectively consists of a single pathway. However, in the remaining 25%, there are 2 different pathways in the node and one conducts electricity faster than the other. Hence they are known as the fast and slow AV nodal pathways.
In a very small number of people with 2 AV nodal pathways, electricity can sometimes go down the slow pathway and then turn around and go back up the fast pathway (and even more rarely the other way around). This sets up an abnormal reentry circuit called AVNRT and causes tachycardia and palpitations. It also occurs in about 1 in every 700 people.
Atrial Tachycardia
Atrial tachycardia can occur at any age and can either be due to a reentry circuit within the left or right atrium or more commonly as a single focus within one of these chambers firing off rapidly. Drugs are often effective for this arrhythmia but ablation can also be performed to cure the problem.
Symptoms
SVTs usually present with rapid, regular palpitations that start and stop suddenly. They can occur at any time of day or night and need not be related to exercise. It is quite common for the rapid palpitations to be associated with shortness of breath or mild chest discomfort. Rarely they can cause black-outs.
Diagnosis
SVT can be diagnosed by recording an ECG during symptoms or from wearing a cardiac monitor. It is not uncommon for it to be difficult to record an episode (as episodes can be infrequent) and so these rhythms can be ‘induced’ during a procedure called an electrophysiology study (or EP study). An EP study is where fine wires are inserted into the heart, via the veins at the top of the leg. The heart can be paced rapidly using these wires to start and stop an SVT. EP studies can be performed in people of any age, from babies to patients >100years old.
Most people with SVT have normal ECGs when they don’t have palpitations. However, if you are born with an accessory pathway, you may have a feature on your ECG called pre-excitation. This feature proves you have an accessory pathway and it is usually possible to identify where it is located in the heart. This only applies to accessory pathways that conduct electricity from the atria to the ventricles. If the pathway only conducts electricity in the other direction (i.e. backwards), it does not show up on an ECG and is known as a concealed accessory pathway.
Treatment
There are broadly three different types of treatment for SVT.
1. Conservative measures – All SVTs, particularly AVRT and AVNRT, may be stopped by performing what is called a Valsalva manoeuvre. This manoeuvre is performed by bearing down (as if going to the toilet) and usually holding one’s breath at the same time. Alternative techniques include blowing into a paper bag or syringe, splashing your face with cold water, drinking ice-cold water, rubbing the side of your neck for 5 seconds or even pressing gently on your eyeballs. It is important a properly trained physician teaches the last two techniques to you. If these manoeuvres are not successful, injection of a drug called adenosine (administered in an A&E department) or verapamil is usually successful at rapidly restoring normal rhythm and is useful in confirming the diagnosis.
2. Anti-arrhythmic drugs – There are various drugs that can be taken to try to prevent episodes of SVT, although they are used infrequently for AVNRT and AVRT where ablation is the norm. Drugs include beta-blockers, verapamil, flecainide, sotalol, propafenone and sometimes amiodarone. They all have different side effect profiles and would usually need to be taken long term. If SVT attacks are rare, it is often not sensible to take a preventative medication every day, so these can be taken as a ‘pill-in-the-pocket’ instead. This means the drug is taken after an attack has started to try and limit its duration. As catheter ablation is so successful for most SVTs, it is not usually necessary for patients to take medications for long periods any more.
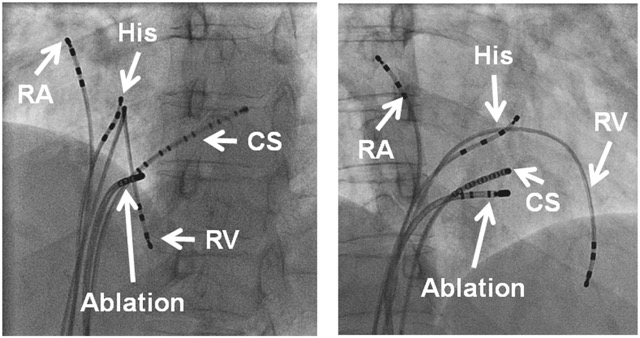
3. Catheter ablation for SVT– Ablation involves a procedure where fine wires are advanced from veins at the top of the leg to the heart. Pacing the heart can then induce SVT. Heat applied from the tip of one of the wires causes a tiny area of localized tissue damage (the tissue is cauterized, or more properly ‘ablated’). This destroys one limb of the abnormal circuit and so cures the arrhythmia. The abnormal limb in AVRT is the accessory pathway, in AVNRT it is the AV nodal slow pathway and in atrial tachycardia the focal spot it is arising from is the abnormality or part of a reentry circuit.
Ablation of SVT has very high success rates – >95% chance of a permanent cure with one procedure, and ablation can be repeated if necessary if it recurs.
The principal risk of ablation in SVT is damage to the normal wiring of the heart (the AV node). If this does not resolve, a pacemaker needs to be implanted to stop the heart from beating too slowly. This is a risk in ablation of AVNRT (the AV nodal slow pathway is always somewhere near the AV node itself) and of accessory pathways or atrial tachycardias that lie close to the AV node. Fortunately, most accessory pathways and atrial tachycardias are not located close to the AV node. The usually quoted risk of AV node damage requiring a pacemaker for SVT ablation is <1% or 1 in 200. Ablation in areas very close to the node may have a risk as high as 2-5%.
Accessory pathways are most often located on the left side of the heart – somewhere along the mitral valve, which lies between the left atrium and left ventricle. A procedure called transseptal puncture is required to access this region with catheters (see figure below). A long metal needle is introduced from the top of the leg into the heart. It is advanced through the wall between the right and left atria (the inter-atrial septum). The hole created allows passage of a long plastic sheath over the needle, which can then be used to introduce an ablation catheter. Risks include making a hole in an outer wall of the heart, leading to blood leaking out into the cavity around the heart, a complication called pericardial tamponade. The risk of this happening is less than 1%. If it occurs, it can usually be successfully treated with temporary insertion of a small tube under the ribs. If this doesn’t work, surgery can be required, but this is very rare. Another theoretical risk of ablating on the left side of the heart is causing a stroke, although this would be exceptionally rare. The hole created in the inter-atrial septum by transseptal puncture usually heals itself. Even if it does not, it does not cause any further problems.
![]()
Wolff-Parkinson-White Syndrome
People born with an accessory pathway which conducts electricity from the atria to the ventricles have an abnormal ECG appearance called pre-excitation. This is because the area of the ventricle connected to the accessory pathway is activated earlier than normal. People with a pre-excited ECG and who also have AVRT are said to have the Wolff-Parkinson-White Syndrome (or WPW for short). People with a pre-excited ECG are often said to have a ‘WPW’ ECG, although this is technically incorrect, as the ECG alone is insufficient to make this diagnosis.
In addition to causing palpitations (the abnormal reentry circuit of AVRT), Wolff-Parkinson-White Syndrome has another important implication. People with accessory pathways are known to occasionally get another rhythm called atrial fibrillation (AF). This is a rapid, chaotic rhythm confined to the atria causing rapid, irregular palpitations. Unlike the AV node, some accessory pathway can conduct electricity very rapidly. This type of pathway will allow lots of the abnormal signals from the atria during an episode of atrial fibrillation to conduct to the ventricles. This is known as pre-excited AF. This rhythm is potentially dangerous as it can degenerate into a lethal heart rhythm called ventricular fibrillation, which causes cardiac arrest and death. This risk is very small, but nevertheless clearly very important. It sometimes means ablation is performed to destroy the pathway even if a patient has never had palpitations or AVRT. This is known as asymptomatic pre-excitation.
The distinction is important as it is known that people with WPW have a slightly higher risk of dying suddenly due to pre-excited AF than people with asymptomatic pre-excitation. For this reason, all people with WPW Syndrome (i.e. patients with pre-excitation and symptoms due to AVRT) are typically offered ablation as first line treatment. If you have asymptomatic pre-excitation, the risk of dying suddenly is thought to be very small indeed, perhaps 1 in every 10,000 people with this condition. An electrophysiology study can be performed to calculate the speed electricity conduct down an accessory pathway in order to determine the future risk of sudden death, although this is not routine. If it conducts very rapidly, ablation may still be performed to prevent pre-excited AF from occurring but it is quite reasonable not to perform an EP study in this setting as the risk of dying is so small.